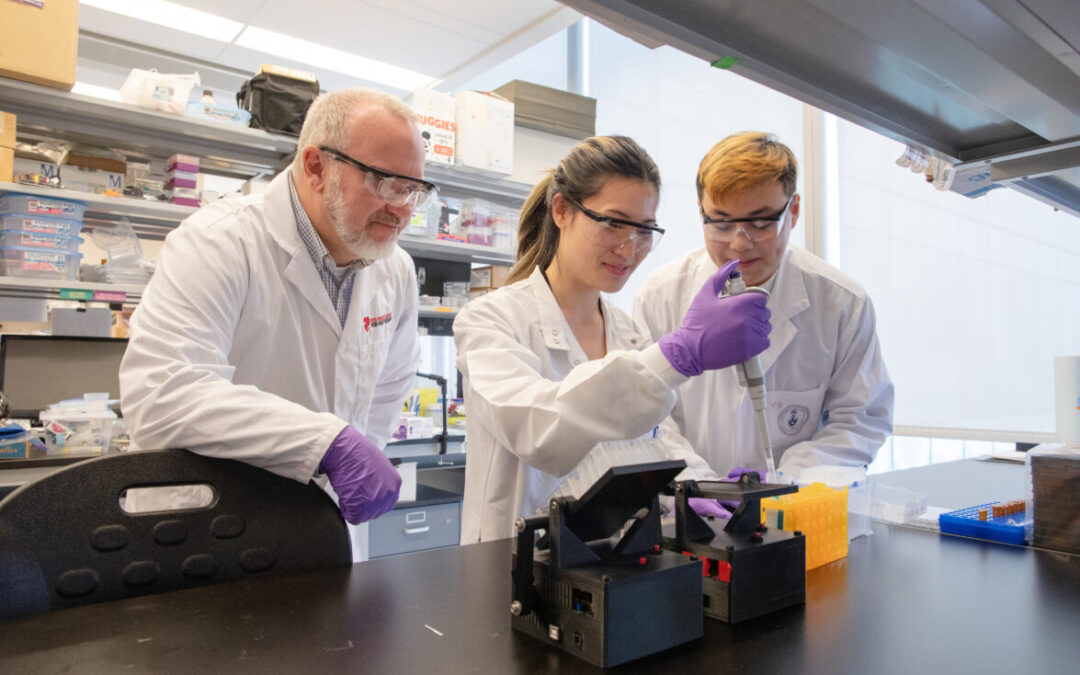
For researchers studying heart disease, lab-grown heart cells are an essential tool. Created from human stem cells, they offer a powerful way to model disease, test therapies, and better understand heart function. However, the challenge remains that these cells behave...
For children living with cardiomyopathy, heart failure is not always caused by the heart losing its ability to pump. In many cases, the problem is more subtle, but just as serious: the heart becomes stiff and struggles to relax and fill properly between beats. This...
New findings from the UNEARTH CVD research team have shed light on an important but often overlooked aspect of cardiovascular care: the cognitive health of people living with heart failure. Published in Cureus, this new publication is the first study to examine...
The Ted Rogers Centre for Heart Research is proud to celebrate an extraordinary milestone in the career of Dr. Paul Santerre, who has been elected as a Fellow of the National Academy of Inventors (NAI), the highest honour bestowed upon academic inventors. This...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
3D models of heart failure… stiffened hearts in diabetes…. saving infant lives
After a heart attack, this peptide protects the heart from further injury
Featured Event
2026 Heart Failure Symposium
Virtual Library
Visit our YouTube channel filled with world-class heart failure educational sessions on diverse topics
Launching in March 2024, emergency department (ED) physicians at the University Health Network (UHN) can now access the Emergency Heart Failure Mortality Risk Grade (EHMRG) calculator within Epic, UHN’s electronic medical record. The EHMRG score estimates the risk of a heart failure patient dying within 7 and 30 days based on 13 key metrics calculated in the ED and supports ED physicians in their decisions of whether to discharge a heart failure patient or admit them to the hospital. Based on the score, different courses of action are recommended depending on a patient’s risk category. The tool was created by Dr. Douglas Lee, a cardiologist at the University Health Network and Chair of Heart Failure Outcomes, and is funded by the Ted Rogers Centre for Heart Research and Institute for Clinical and Evaluative Sciences (ICES). The Epic integration at UHN is the first in Canada for this decision-support tool.
Dr. Sam Sabbah, UHN Chief of the Department of Emergency Medicine, has been excited to see the tool’s trajectory so far. “UHN Emergency Department clinicians enrolled patients into the COACH trial and contributed to the development and validation of the score. Fast forward all these years, it’s now becoming a best practice and is integrated into our workflow in Epic—let’s take a moment to celebrate that.”
EMHRG provides a low-, intermediate-, or high-risk score based on the patient’s presenting metrics, such as their age, whether they arrived by ambulance, their blood pressure, their creatinine, and their potassium levels. Low-risk patients can be safely discharged from the hospital and given a follow-up appointment with a heart function clinic within two weeks. High-risk individuals should be admitted to the hospital from the emergency department for immediate care and ongoing monitoring. An intermediate score prompts further consultations with hospital specialists to determine if they should discharge the patient and have them return to the hospital for a follow-up within a few days or admit the patient for monitoring.
The EHMRG Calculator provides a low, intermediate, or high score depending on the patient’s presenting metrics.
The EHMRG calculator’s benefits extend beyond just individual patients, however. It supports clinical decision-making with an objective and evidence-based score—generated automatically and quickly—to help ensure the safety of patients and efficiency of the workflow in a busy ED. This improves patient quality of life, ensures allocation of hospital resources to those in most critical need, and reduces healthcare expenses.
“In the fast-paced environment of emergency rooms, where decisions can mean the difference between life and death, the Emergency Heart Failure Mortality Risk Grade (EHMRG) score provides timely insights to help make the right decision. Heart failure is complex, and objective measures like the EHMRG score can complement physician clinical judgment,” explains Dr. Douglas Lee, the visionary behind the EHMRG calculator. “By integrating this calculator into the Epic system at UHN, we’re not just enhancing the decision-making process, we’re helping to transform the way heart failure is managed in the emergency department. It’s a step forward in our mission to improve the quality of care for heart failure patients across the province.”
The EHMRG Calculator is now live in Epic’s electronic medical record system across the University Health Network.
Before receiving the greenlight for integration into Epic, the EHMRG score was first validated in a large trial with ten hospitals in Ontario. In the Comparison of Outcomes and Access to Care for Heart Failure (COACH) trial published in the New England Journal of Medicine, over 5,000 patients who came to the emergency department with acute heart failure were divided into two groups. One received usual care, and the other received a special hospital-based strategy using the EHMRG calculator to help physicians determine which patients were able to be safely discharged with follow-up.
The results showed that within 30 days of receiving treatment, the group using the EHMRG calculator had a lower rate of either dying from any cause or being hospitalized again for heart problems (12.1%) compared to the group that received usual care (14.5%). Over 20 months, the difference in health outcomes between the two groups continued to be better for the EHMRG care group. Specifically, only the patients in the EHMRG group experienced a statistically significant reduction in death or repeat hospitalization for cardiovascular reasons compared to the control group.
The study concluded that for patients with acute heart failure, receiving care informed by their individual risk level calculated with the EHMRG score in tandem with rapid follow-up at a heart function clinic resulted in a lower risk of mortality or rehospitalization. It was this promising result that led the Epic and UHN teams to design an integrated care pathway for the ED that incorporated the EHMRG score and integrated it into Epic at multiple UHN sites. This is just the latest TRCHR tool to be integrated for wide-scale use across hospitals, showcasing the incredible impact of both the research and translational work being done by the scientists and clinicians at TRCHR.