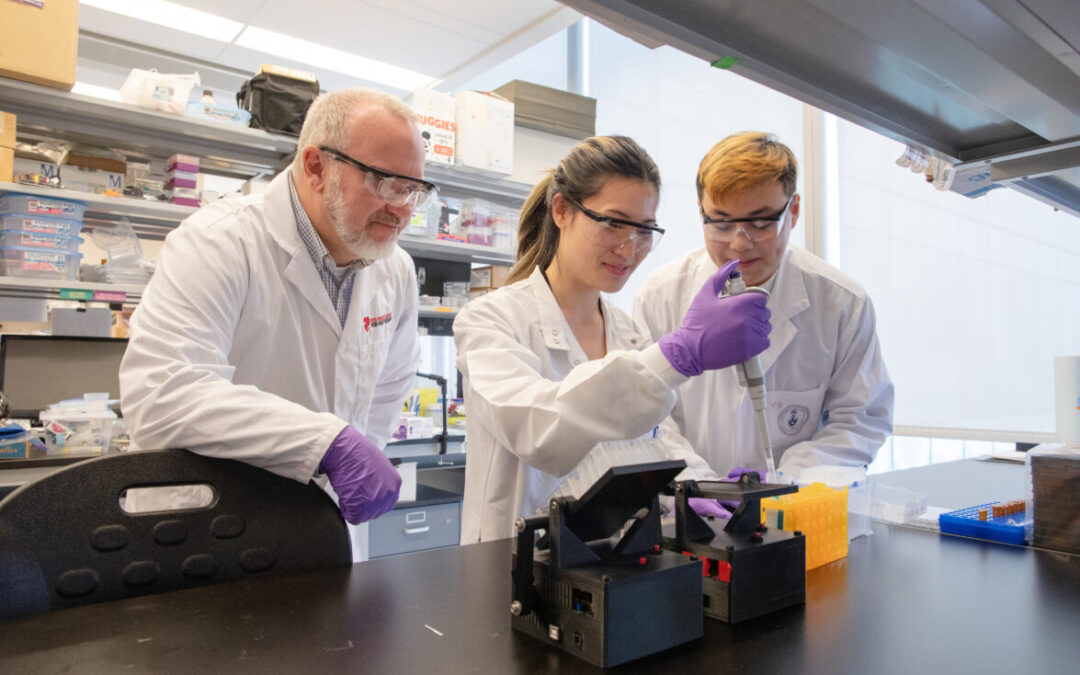
For researchers studying heart disease, lab-grown heart cells are an essential tool. Created from human stem cells, they offer a powerful way to model disease, test therapies, and better understand heart function. However, the challenge remains that these cells behave...
For children living with cardiomyopathy, heart failure is not always caused by the heart losing its ability to pump. In many cases, the problem is more subtle, but just as serious: the heart becomes stiff and struggles to relax and fill properly between beats. This...
New findings from the UNEARTH CVD research team have shed light on an important but often overlooked aspect of cardiovascular care: the cognitive health of people living with heart failure. Published in Cureus, this new publication is the first study to examine...
The Ted Rogers Centre for Heart Research is proud to celebrate an extraordinary milestone in the career of Dr. Paul Santerre, who has been elected as a Fellow of the National Academy of Inventors (NAI), the highest honour bestowed upon academic inventors. This...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
3D models of heart failure… stiffened hearts in diabetes…. saving infant lives
After a heart attack, this peptide protects the heart from further injury
Featured Event
2026 Heart Failure Symposium
Virtual Library
Visit our YouTube channel filled with world-class heart failure educational sessions on diverse topics
Investigating Heart Failure
Personalized Medicine
Equitable Access to Care
Translating Innovation
For Patients
For Clinicians
For Researchers
Study reveals inequitable COVID-19 infection rates from the very beginning
In a new study published in Nature Scientific Reports, supported by a Ted Rogers Centre Innovation Fund grant, collaborators sought to understand if public health efforts helped reduce the risk of SARS-CoV-2 infection among those whose sociodemographics and health conditions made them more vulnerable.
The focus was Ontario, with a large population, tremendous diversity, and a robust system of population data in place courtesy of ICES.
The Challenge
In the pandemic’s early days, there was a lack of evidence around what put patients at higher risk for COVID-19. In this study, researchers sought local data to gain context on what were true, adjusted risk factors for infection.
“We were also curious to see, during the peak of the first wave, how non-pharmaceutical public health interventions such as masking were influencing risk among different communities,” says University of Toronto MD/PhD candidate Bahar Behrouzi and a lead author on the paper. “We suspected that these interventions weren’t helping everyone equitably.”
The study was among the world’s most rigorous to assess COVID-19’s impact at the level of race, ethnicity, and other socioeconomic determinants of health. What we would learn in the first few months of the pandemic yields important lessons for the future.
The Study
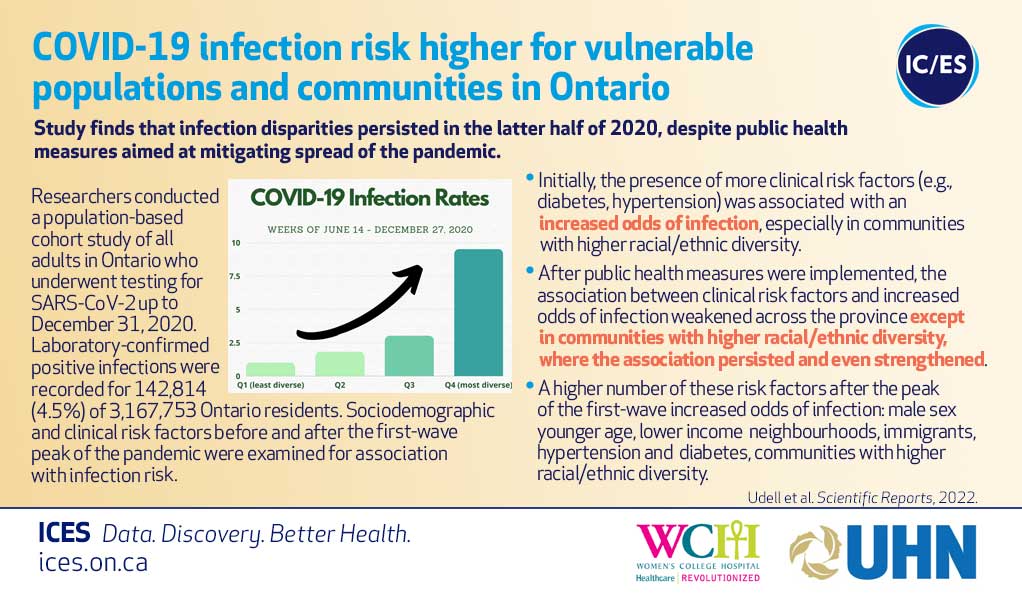
Ontario entered a province-wide lockdown after the first wave of COVID-19 peaked in April 2020. Researchers found that, initially, the following clusters of people had the highest infection rates:
Older adults
Men
Immigrants
Those with hypertension and diabetes
Those living in the most ethnically diverse urban areas
Those living in the most socioeconomically disadvantaged communities
After the initial COVID-19 surge, the link between age and infection risk reversed toward younger adults. But all other risk factors persisted throughout 2020, most notably in the communities with the greatest degrees of racial or ethnic diversity.
“After the first-wave peak, interventions such as masks, social distancing and stay-at-home orders reduced infection rates overall, but it was striking to see how much less of an impact they had in neighbourhoods with higher proportions of visible minorities,” says Bahar, who also earned a Ted Rogers Centre Education Fund award for her work.
Not everyone, as we know, is able to shelter in place or work from home.
What it Means
While it became apparent as the pandemic wore on that these neighbourhoods were not being equitably protected from COVID-19, this study shows that the disparity happened right at the very beginning.
“You’d tend to expect everyone would reap the benefits of universal measures to curb the spread of COVID-19, but this study helps highlight that is simply not the case,” Bahar says. “What we can learn is that for the next health crisis, we need solutions built from an equitable standpoint, perhaps improved sick day policies and better access to testing in more vulnerable communities.”
By assessing what actually happened in Ontario when SARS-CoV-2 struck, we can take action and develop proactive plans to ensure that the most vulnerable people are as safe as anyone – and build a more resilient health system in the process.
***
Collaborating researchers on the study are from: ICES, Women’s College Hospital, U of T’s Institute of Health Policy, Management, and Evaluation, U of T Medicine, UHN, St. Michael’s Hospital, Canadian VIGOUR Centre, University of Alberta, Western University of Health Sciences (Pomona, CA), and Sunnybrook.