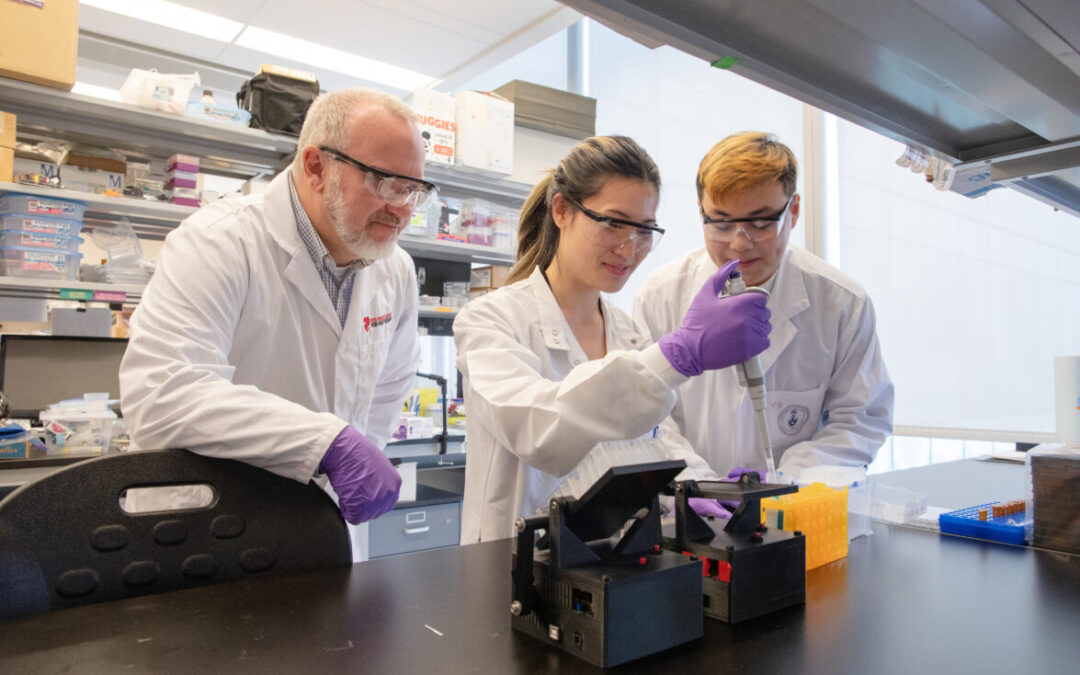
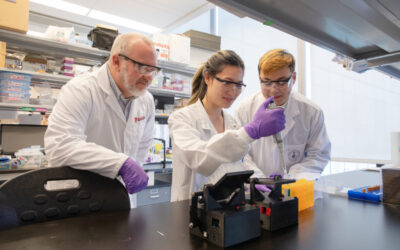
For researchers studying heart disease, lab-grown heart cells are an essential tool. Created from human stem cells, they offer a powerful way to model disease, test therapies, and better understand heart function. However, the challenge remains that these cells behave...
For children living with cardiomyopathy, heart failure is not always caused by the heart losing its ability to pump. In many cases, the problem is more subtle, but just as serious: the heart becomes stiff and struggles to relax and fill properly between beats. This...
New findings from the UNEARTH CVD research team have shed light on an important but often overlooked aspect of cardiovascular care: the cognitive health of people living with heart failure. Published in Cureus, this new publication is the first study to examine...
The Ted Rogers Centre for Heart Research is proud to celebrate an extraordinary milestone in the career of Dr. Paul Santerre, who has been elected as a Fellow of the National Academy of Inventors (NAI), the highest honour bestowed upon academic inventors. This...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
3D models of heart failure… stiffened hearts in diabetes…. saving infant lives
After a heart attack, this peptide protects the heart from further injury
Featured Event
2026 Heart Failure Symposium
Virtual Library
Visit our YouTube channel filled with world-class heart failure educational sessions on diverse topics
Investigating Heart Failure
Personalized Medicine
Equitable Access to Care
Translating Innovation
For Patients
For Clinicians
For Researchers
New tool to help doctors better prevent sudden cardiac death in children
In a new study published in Circulation, a Ted Rogers Centre for Heart Research team has proven that a digital tool developed at The Hospital for Sick Children can successfully identify pediatric cardiomyopathy patients who are at high risk for sudden cardiac death.
This risk prediction “calculator”, two years in the making, was tested and validated in 570 children with hypertrophic cardiomyopathy (HCM) at 20 of the world’s leading children’s hospitals. It proved to be over 70% accurate in distinguishing those children at greater risk of the most tragic outcome. The tool is called “Precision Medicine for Cardiomyopathy” or simply PRIMaCY.
HCM is a genetic disease, marked by a thickened heart muscle, that is a leading cause of sudden cardiac death in adolescents and young adults. To prevent such outcomes, hospitals use implantable cardioverter-defibrillator (ICD) devices to detect and stop dangerously abnormal heartbeats.
For child patients, however, there had previously been no way to accurately determine who is facing a heightened risk of sudden death – and who needs an ICD right away. Not knowing has resulted in tragic, unnecessary deaths as well as devices implanted in children who don’t need them, exposing them to potential complications.
“In pediatric heart failure, there is a huge gap in knowledge that has interfered with our ability to prevent these outcomes, resulting in unnecessary use of ICDs,” says Dr. Seema Mital, head of cardiovascular research at SickKids and Ted Rogers Centre scientific lead.
“Our risk model is the first to be validated in a pediatric population, and is driven by factors unique to child patients. It is a much-needed precision strategy to prevent sudden cardiac death and make informed decisions on the use of ICDs.”
Dr. Seema Mital
Data-backed decisions that are individualized, not generic
Whether or not to place an ICD in a young patient is a complex discussion between physicians and families. This new tool supports this shared decision-making, providing an individual risk score rather than more arbitrary “high” and “low” risks that are hard to interpret. It does so by combining many risk factors – for example, a child’s age, medical history, family history, and measurements from diagnostic tests such as echocardiogram – to create an objective risk of sudden death in coming years.
Instead of a one-size-fits-all approach, the tool can help people make decisions based on their individual risk tolerance. Each family can debate risks and benefits of an ICD placement with their doctors, and take a fully informed approach to their child’s treatment.
Importantly, this calculator will be built as a digital tool to embed in a hospital’s electronic health records (EMRs). From there, it will extract clinical, physiological, environmental and lifestyle data on each patient to generate a risk score that physicians and families can trust. Being a part of EMRs means health-care teams can also document progress over time that could reveal important new clinical clues.
Over the next six months, SickKids staff will pilot the tool in clinical practice. If the team is confident it is serving the right patient populations, they will offer it first to all hospitals who were part of the study.
Eventually, any centre with a health record system can deploy this calculator – and bring greater precision to the practice of saving lives of children with heart failure.
* * *
Collaborating pediatric centres:
Canada
BC Children’s Hospital
Children’s Hospital of Eastern Ontario
The Hospital for Sick Children
Stollery Children’s Hospital
United States
Boston Children’s Hospital
Brigham and Women’s Hospital
C.S. Mott Children’s Hospital
Children’s Medical Centre of Dallas
Children’s Healthcare of Atlanta
Children’s Hospital Colorado
Children’s Hospital of Los Angeles
Children’s Hospital of Philadelphia
Cincinnati Children’s Hospital
Cleveland Clinic Children’s Hospital
Johns Hopkins Medical Center
Lucile Packard Children’s Hospital
Medical University of South Carolina
Monroe Carrell Jr. Children’s Hospital
Morgan Stanley Children’s Hospital
OHSU Doernbecher Children’s Hospital
Riley Children’s Hospital
Texas Children’s Hospital
University of Tennessee Health Science Center
University of Utah Primary Children’s Hospital
Australia
Agnes Ginges Centre for Molecular Cardiology at Centenary Institute The University of Sydney
Murdoch Children’s Research Institute, University of Melbourne
The Royal Children’s Hospital
Netherlands
Department of Cardiology, Thoraxcenter, Erasmus MC Rotterdam
Italy
Careggi University Hospital
Brazil
Heart Institute (InCor), University of Sao Paulo Medical School