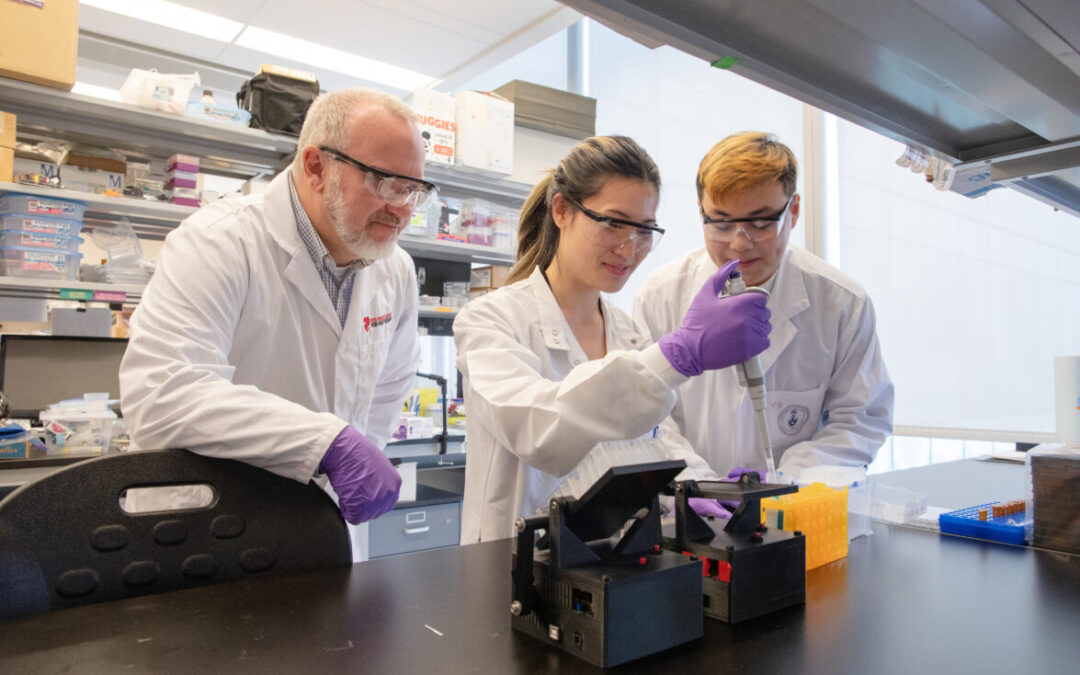
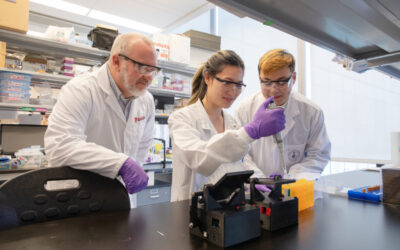
For researchers studying heart disease, lab-grown heart cells are an essential tool. Created from human stem cells, they offer a powerful way to model disease, test therapies, and better understand heart function. However, the challenge remains that these cells behave...
For children living with cardiomyopathy, heart failure is not always caused by the heart losing its ability to pump. In many cases, the problem is more subtle, but just as serious: the heart becomes stiff and struggles to relax and fill properly between beats. This...
New findings from the UNEARTH CVD research team have shed light on an important but often overlooked aspect of cardiovascular care: the cognitive health of people living with heart failure. Published in Cureus, this new publication is the first study to examine...
The Ted Rogers Centre for Heart Research is proud to celebrate an extraordinary milestone in the career of Dr. Paul Santerre, who has been elected as a Fellow of the National Academy of Inventors (NAI), the highest honour bestowed upon academic inventors. This...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
3D models of heart failure… stiffened hearts in diabetes…. saving infant lives
After a heart attack, this peptide protects the heart from further injury
Featured Event
2026 Heart Failure Symposium
Virtual Library
Visit our YouTube channel filled with world-class heart failure educational sessions on diverse topics
Investigating Heart Failure
Personalized Medicine
Equitable Access to Care
Translating Innovation
For Patients
For Clinicians
For Researchers
The new heart risk factor we must all begin to consider
For 50 years, physicians and scientists made great strides managing key risk factors for heart disease – high cholesterol, hypertension, smoking, for starters. But the burden of cardiovascular disease, especially its effect on mortality, remains an almost unrivaled public health challenge.
What may we have missed along the way? Only in the past five years has a new, potentially major risk factor drifted into focus: clonal hematopoiesis. This is a phenomenon that can occur in an aging body, where blood cells begin to mutate and form new, genetically different cells.
A new paper published this week in JAMA Cardiology, anchored by our cardiotoxicity prevention program lead Dr. Dinesh Thavendiranathan, provides new context for clonal hematopoiesis by describing its links to heart to disease and to cancer – a field where researchers first discovered it. This paper is novel as, for the first time, it describes clonal hematopoiesis as a potential driver of cardiovascular disease in cancer survivors.
A new risk factor emerges
“Much of the discovery behind clonal hematopoiesis was unexpected,” says Dr. Thavendiranathan, a cardiologist at the Peter Munk Cardiac Centre. “In patients with leukemia, researchers started to see mutations occur in non-leukemia cells – those that happen as we grow older rather than passed down through genes.”
Before clonal hematopoiesis (CH) even had a name, researchers theorized that these mutated cells – which they also spotted in white blood cells of healthy adults – were likely precursors to cancer. Yet, patients with mutations were dying not of cancer but, instead, of heart disease.
That CH may in fact be a cardiac risk factor became more intriguing when the New England Journal published a 2014 paper showing that the risk of vascular disease, stroke or heart attack in people with CH was equivalent to those with high blood pressure or diabetes. It hypothesized that CH is linked to a higher risk of mortality “due to an increased risk of cardiovascular disease.”
Dr. Thavendiranathan analyzes data inside our cardiotoxicity program
“I think that’s where it hit home, because as cardiologists, we see patients who are young, free of diabetes, hypertension and high cholesterol, but still they’ve had a heart attack,” says Dr. Thavendiranathan. “And there are people whose various health conditions are well managed but they have a heart attack. There are clearly other risk factors at play for cardiovascular disease.”
A flurry of studies have emerged in the last few years further exploring CH as a cardiac risk factor, including a 2017 study showing twice the risk of coronary heart disease in humans. Many leaders in the field are now rushing to address this important issue.
Where do we go from here?
The new collaborative paper, with lead author Dr. Oscar Calvillo (a fellow in the Centre’s cardiotoxicity program), Dr. Thavendiranathan, and several global leaders in the field, further highlights CH as an emerging, important area of focus in the interconnected world of cancer and heart disease. While we must sort out the mechanisms of how it does so, CH appears to have specific consequences: a higher risk of malignant conditions such as leukemia, but also ischemic stroke, early heart attacks and coronary heart disease.
“Our paper suggests that cardiologists should be familiar with clonal hematopoiesis, because evidence shows it is linked to a greater risk of cardiovascular disease,” says Dr. Thavendiranathan. “We also see that CH is linked to cancer, so we now have a shared risk factor for the two major diseases. This also means CH is something we must watch for when patients receive cancer therapy, as it may drive the toxic effects on the heart.”
He says that by age 70, one in 10 adults will have CH – yet deeper analysis may make this number run higher. It is a field now of discovery, and of questions: Who should be screened for CH? How often? When should doctors intervene with therapy? What therapy?
As part of the Centre’s cardiotoxicity program, there is now a clinic at Peter Munk Cardiac Centre devoted to clonal hematopoiesis. Clinician-scientist Aaron Schimmer at Princess Margaret Cancer Centre is helping develop an inexpensive assay that could be used to measure CH levels in patients. When it emerges, expected within two years, Dr. Thavendiranathan expects the number of patients in this clinic to rise sharply.
Overall, typical heart health screenings in the near future may not only target weight, cholesterol, blood glucose and LDL cholesterol, but also clonal hematopoiesis.