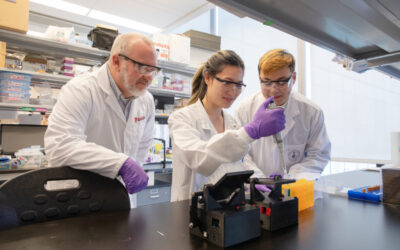
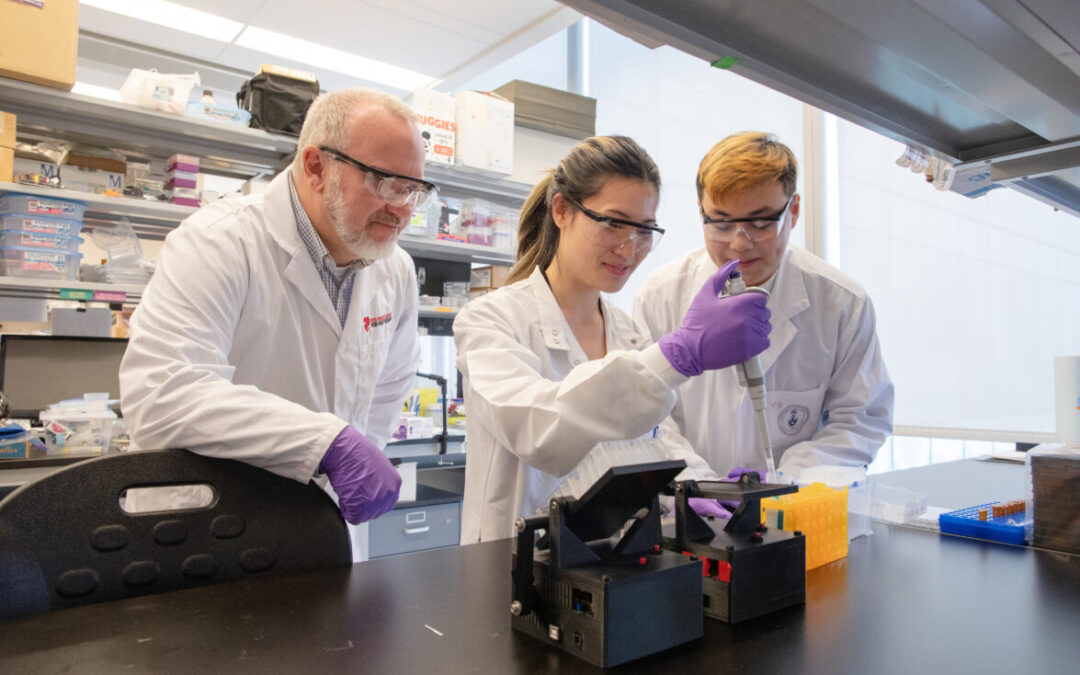
For researchers studying heart disease, lab-grown heart cells are an essential tool. Created from human stem cells, they offer a powerful way to model disease, test therapies, and better understand heart function. However, the challenge remains that these cells behave...
For children living with cardiomyopathy, heart failure is not always caused by the heart losing its ability to pump. In many cases, the problem is more subtle, but just as serious: the heart becomes stiff and struggles to relax and fill properly between beats. This...
New findings from the UNEARTH CVD research team have shed light on an important but often overlooked aspect of cardiovascular care: the cognitive health of people living with heart failure. Published in Cureus, this new publication is the first study to examine...
The Ted Rogers Centre for Heart Research is proud to celebrate an extraordinary milestone in the career of Dr. Paul Santerre, who has been elected as a Fellow of the National Academy of Inventors (NAI), the highest honour bestowed upon academic inventors. This...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
3D models of heart failure… stiffened hearts in diabetes…. saving infant lives
After a heart attack, this peptide protects the heart from further injury
Featured Event
2026 Heart Failure Symposium
Virtual Library
Visit our YouTube channel filled with world-class heart failure educational sessions on diverse topics
Investigating Heart Failure
Personalized Medicine
Equitable Access to Care
Translating Innovation
For Patients
For Clinicians
For Researchers
How cardiac imaging, biomarkers could improve cancer care
In early June, Dr. Dinesh Thavendiranathan, Ted Rogers Centre investigator and lead of our cardiotoxicity prevention program, presented at the ASCO annual meeting in Chicago. We republish this story courtesy of TriMed Media Group. It was originally published here.
*****
by Melissa Rohman, TriMed Media
Dinesh Thavendiranathan, MD, a scientist at the Toronto General Hospital Research Institute, discussed how cardiac imaging and biomarkers can significantly improve cancer patient care at this year’s American Society of Clinical Oncology (ASCO)’s annual meeting.
Dr. Thavendiranathan believes cardiac imaging and biomarkers will help physicians perform pre-treatment risk and assessment of heart failure, make early detections of myocardial injury during cancer therapy and identify subclinical myocardial disease in cancer survivors.
“I believe that in next five to ten years, we’re going to be seeing studies about this being published and hopefully some of them will show what we can truly to do change the outcomes of cancer patients and change the way we follow our patients during cancer therapy,” Dr. Thavendiranathan said.
Cancer patients at risk of heart failure
Measuring left ventricular ejection fraction (LVEF) with echocardiography or myocardial strain/deformation imaging are the most useful methods for pre-treatment risk assessment in cancer patients at risk of developing heart failure.
“We know that in anthracycline treated patients who have the initiation of cancer therapy are subsequently at higher risk of symptomatic heart failure,” Dr. Thavendiranathan said. “Patients who have below normal or mildly reduced ejection fraction at the initiation of cancer therapy are at a significantly higher risk of symptomatic heart failure; patients who are receiving low dose anthracyclines or trastuzumab can be considered at an elevated risk for heart failure. Imaging can play an important role.”
Echocardiography
Dr. Thavendiranathan (pictured at right) said with echocardiography, LVEF can be measured in two different ways: using 2D or 3D imaging techniques, though 3D imaging has proven to be more accurate and precise than 2D and as accurate as MUGA (multigated acquisition) scans.
However, due to repeated exposure to radiation and that a MUGA scan only provides an assessment of ejection fraction, Dr. Thavendiranathan claimed the industry has moved away from ejection fraction to measure myocardial myopathy and using myocardial strain imaging instead to monitor a patient during cancer therapy.
Myocardial strain imaging and biomarkers
A less popular form of cardiac imaging, myocardial strain imaging looks beyond the translation of the borders of the heart to measure myocardial deformation and could be a better marker for myocardial myopathy than ejection fraction, Dr. Thavendiranathan said.
“When there’s a new technique that’s introduced, there’s always a bit of trepidation and I want to reassure you that strain measurements are not really more complex than ejection fraction measurements,” he said.
Additionally, serum biomarkers can improve the results of cardiac imaging, though timing, assay use and thresholds must be defined for accurate and high-quality results.
Will it actually help?
For example, when identifying cancer patients who are transitioning from stage A heart failure (patients who are high risk, but show no symptoms) to stage B heart failure (patients with structural heart abnormalities, but show no symptoms), will cardiac imaging and biomarkers help? According to Dr. Thavendiranathan, the answer is yes.
With the help of biomarkers, 3D myocardial imaging can detect changes in EF earlier than 2D imaging and 3D echocardiography also has shown to better detect LVEF at a 50 percent threshold than 2D imaging, he said.







 Dr. Thavendiranathan (pictured at right) said with echocardiography, LVEF can be measured in two different ways: using 2D or 3D imaging techniques, though 3D imaging has proven to be more accurate and precise than 2D and as accurate as MUGA (multigated acquisition) scans.
Dr. Thavendiranathan (pictured at right) said with echocardiography, LVEF can be measured in two different ways: using 2D or 3D imaging techniques, though 3D imaging has proven to be more accurate and precise than 2D and as accurate as MUGA (multigated acquisition) scans.