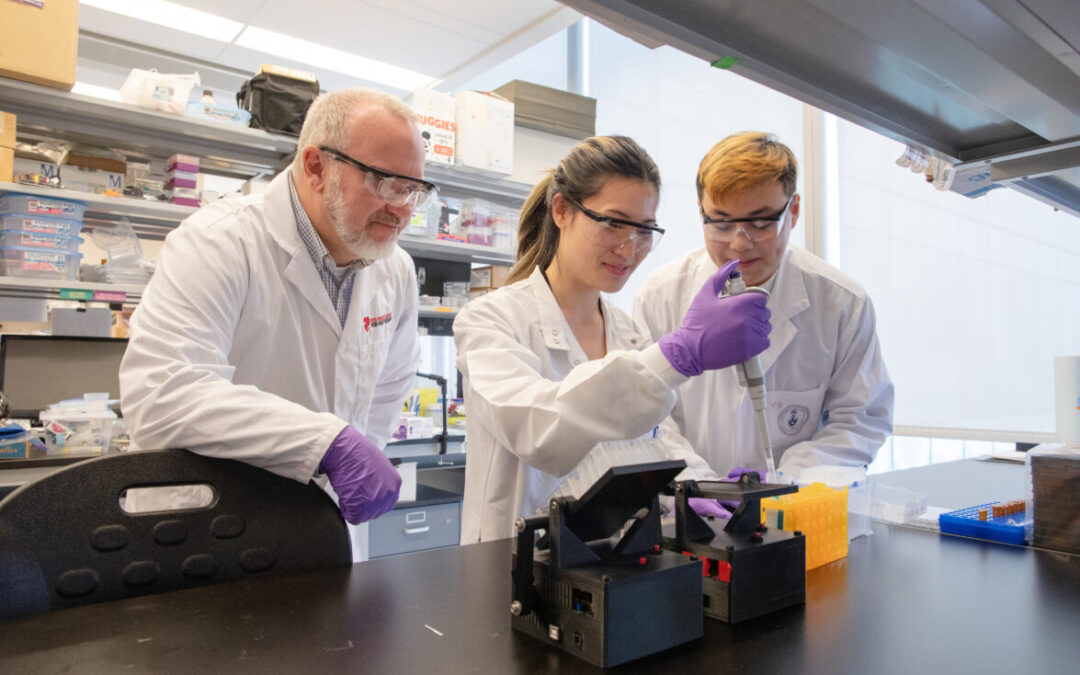
For researchers studying heart disease, lab-grown heart cells are an essential tool. Created from human stem cells, they offer a powerful way to model disease, test therapies, and better understand heart function. However, the challenge remains that these cells behave...
For children living with cardiomyopathy, heart failure is not always caused by the heart losing its ability to pump. In many cases, the problem is more subtle, but just as serious: the heart becomes stiff and struggles to relax and fill properly between beats. This...
New findings from the UNEARTH CVD research team have shed light on an important but often overlooked aspect of cardiovascular care: the cognitive health of people living with heart failure. Published in Cureus, this new publication is the first study to examine...
The Ted Rogers Centre for Heart Research is proud to celebrate an extraordinary milestone in the career of Dr. Paul Santerre, who has been elected as a Fellow of the National Academy of Inventors (NAI), the highest honour bestowed upon academic inventors. This...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
3D models of heart failure… stiffened hearts in diabetes…. saving infant lives
After a heart attack, this peptide protects the heart from further injury
Featured Event
2026 Heart Failure Symposium
Virtual Library
Visit our YouTube channel filled with world-class heart failure educational sessions on diverse topics
Investigating Heart Failure
Personalized Medicine
Equitable Access to Care
Translating Innovation
For Patients
For Clinicians
For Researchers
‘FREEDOM’ from multivessel disease: new study confirms bypass surgery is ideal treatment
Two years ago, a landmark clinical trial called “FREEDOM” sought answers to a clinical problem that had long been unclear to cardiologists: how to most effectively reopen blocked blood vessels in the heart in patients with diabetes who have multiple blockages. This is known as coronary revascularization.
FREEDOM’s important finding was that coronary artery bypass grafting (CABG) was superior to percutaneous coronary intervention (PCI, commonly known as stenting) by improving long-term survival. Still, this occurred in a carefully controlled setting – results were yet to be seen in the real world of patient care.
A new study led by Dr. Douglas Lee, Ted Rogers Centre Chair in Heart Function Outcomes, used one decade of data from about 14,000 patients in Ontario to address this knowledge gap. What researchers found points to important considerations for both those performing these procedures and the patients receiving them. It has just been published in the Journal of the American College of Cardiology.
Deep pool of data confirms answers
Across 11 cardiac surgery centres in Ontario, Dr. Lee’s team compared early and long-term outcomes in CABG (a more invasive approach) and PCI (a less invasive approach) in patients with diabetes and multivessel disease from 2007 to 2016. To ensure a fully equal and fair comparison, they used a statistical technique called “propensity score matching” to identify 4,300 pairs of patients that closely resembled each other for age and health status.
The study revealed that, in these actual clinical settings, patients treated by PCI had higher rates of adverse events and mortality six to 10 years later. This finding, which supports the FREEDOM results, is the subject of a “blockbuster” oral presentation at the world’s largest cardiology meeting, the 2020 ESC Congress.
“Our study suggests that bypass surgery is a more durable repair option for these patients and it should be considered the treatment of choice in patients with diabetes and multivessel disease that are good surgical candidates,” says Dr. Derrick Tam, a resident in cardiac surgery at U of T and first author of the paper.
Studies like this, using a deep pool of data, can be done in very few places around the world, Dr. Tam says. This study leveraged Ontario population data from ICES and the CorHealth Registry, through which researchers could follow every single patient over the long-term – including those who died.
Collective decisions key to positive outcomes
This study has demonstrated that patients with diabetes and multivessel disease should preferentially be treated with CABG. For cardiologists, it’s a reminder that they may consider referring patients to a cardiac surgeon for a further opinion. In fact, by analyzing surgery billing codes, the study revealed that fewer than 10 per cent of patients who underwent the PCI procedure – less invasive, but less effective over the long term – had any cardiac surgical consult at all.
Listen to a Journal of the American College of Cardiology podcast on this study
“This suggests that as clinicians, we aren’t doing enough in terms of making decisions in a comprehensive, multidisciplinary fashion,” says Dr. Douglas Lee, also cardiologist at Peter Munk Cardiac Centre and senior scientist at ICES. “In another study using this same dataset, we also see that in hospitals that don’t offer cardiac surgery, patients are more likely to have PCI despite having multivessel disease and diabetes. This, as we know now, may not be the appropriate treatment.”
Because diabetes impacts the walls and inner lining of blood vessels, patients more often develop coronary disease and thus require bypass surgery or stenting. After this intervention, their disease can also worsen more quickly than those without diabetes. This may speak to why bypass surgery (CABG) is a more durable option because it not only treats the current blockages, but potentially future ones as well.
“Overall, it’s important for patients to understand all risks and benefits of these interventions as part of a frank, balanced discussion with their cardiology team,” Dr. Lee says.