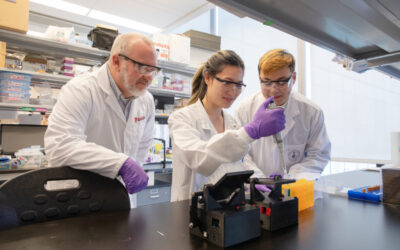
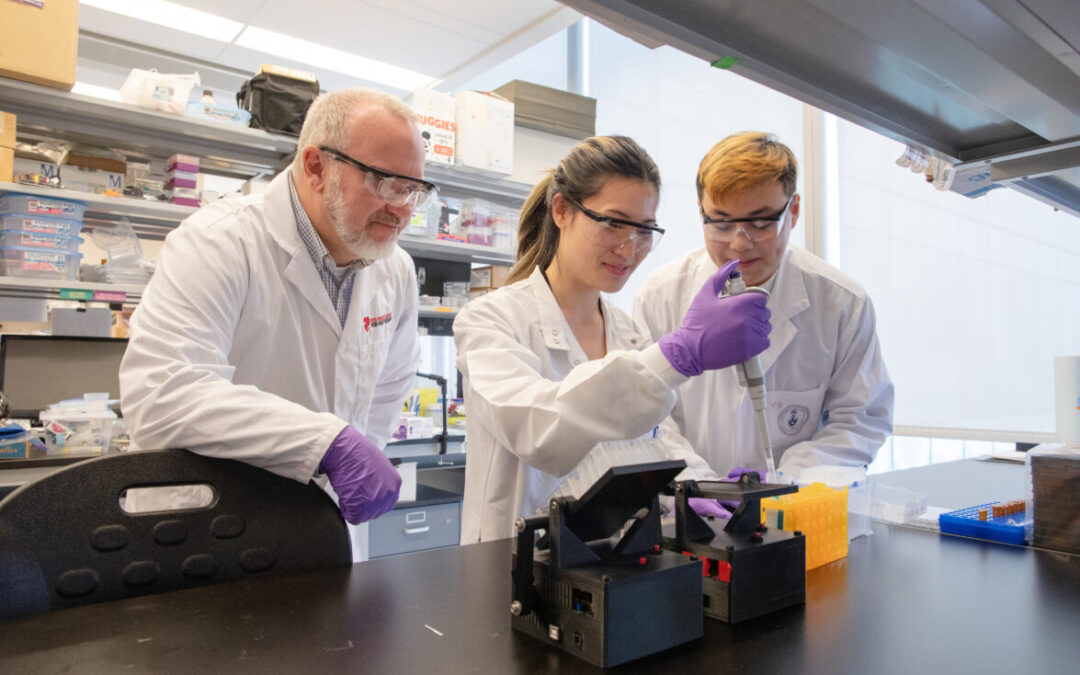
For researchers studying heart disease, lab-grown heart cells are an essential tool. Created from human stem cells, they offer a powerful way to model disease, test therapies, and better understand heart function. However, the challenge remains that these cells behave...
For children living with cardiomyopathy, heart failure is not always caused by the heart losing its ability to pump. In many cases, the problem is more subtle, but just as serious: the heart becomes stiff and struggles to relax and fill properly between beats. This...
New findings from the UNEARTH CVD research team have shed light on an important but often overlooked aspect of cardiovascular care: the cognitive health of people living with heart failure. Published in Cureus, this new publication is the first study to examine...
The Ted Rogers Centre for Heart Research is proud to celebrate an extraordinary milestone in the career of Dr. Paul Santerre, who has been elected as a Fellow of the National Academy of Inventors (NAI), the highest honour bestowed upon academic inventors. This...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
3D models of heart failure… stiffened hearts in diabetes…. saving infant lives
After a heart attack, this peptide protects the heart from further injury
Featured Event
Clinical Cardiology & Critical Care Update
Virtual Library
Visit our YouTube channel filled with world-class heart failure educational sessions on diverse topics
Investigating Heart Failure
Personalized Medicine
Equitable Access to Care
Translating Innovation
For Patients
For Clinicians
For Researchers
Why we must screen early in life for hypertrophic cardiomyopathy
The most common genetic heart disorder is hypertrophic cardiomyopathy (HCM), a disease that risks sudden death in children and in older adults.
“Once a patient is diagnosed, it’s important to screen first-degree relatives as well because the condition can often be silent, with no apparent symptoms,” says Dr. Seema Mital, scientific lead, Ted Rogers Centre.
In clinical screening, an echocardiogram is typically used to detect HCM, where a thickened heart has an impaired ability to pump blood properly. Meanwhile, genetic screening can test family members for the same gene defect found in their relative with HCM. This type of proactive management can save lives.
Yet guidelines from both the European Society of Cardiology (ESC) and American College of Cardiology (ACC) currently state we should routinely screen only those family members who are at least 10 and 12 years old, respectively.
Dr. Mital hopes to change this thinking so that kids of any age can be proactively monitored for a thickened heart. She anchored a new study at SickKids that may impel this shift, one published in the prestigious European Heart Journal.
Why young children must be screened
In that study, researchers screened 524 children with cardiomyopathy, 331 of whom were under the age of 10. With echocardiograms done at all ages, they had significant data available from infants through to 18 years old.
“We found a similar disease occurrence in children under 10 as over 10,” says Dr. Mital, head of cardiovascular research at SickKids. “For all elements of hypertrophic cardiomyopathy – frequency of disease, number of sudden death events, need for an ICD, need for surgery – there were similar results regardless of age.”
In the study, 53% of those screened showed disease before they turned 10 – and what’s more is that the HCM seemed to progress quickly early in life. Before turning 10, 41% of these young patients had a major intervention (ICD, surgery) or experienced, tragically, sudden death.
“This means there is no justification to wait until the age of 10 or 12 before screening children for HCM after a family member is diagnosed,” says Dr. Mital. “It also highlights the need to closely monitor these children in order to perform interventions before a serious complication occurs. If we restrict the starting age for screening, we miss patients whose lives may have been saved had they been diagnosed earlier.”
‘A disease of all ages’
Their new study exposed another important gap in the current guidelines.
Globally, there persists the idea that genetic screening is unnecessary in children under 10. Yet knowing whether one does or does not carry the gene defect that runs in the family can help decide who needs ongoing medical follow-up because of a risk for HCM, and who does not need any further follow-up because they don’t carry that defect.
Removing uncertainty for the future not only helps families cope but saves health-care costs by reducing the unnecessary clinical testing of healthy individuals. Further, Ted Rogers Centre genetic experts have shown that genetic differences can explain why HCM can present much differently in members of the same family. If one person develops a late-onset disease, you can’t make the assumption that will be true of his or her relatives.
“For both clinical and genetic screening, we feel that our data support the idea that these should be offered at any age,” says Dr. Mital. “This is a disease of all ages.”
Early diagnosis saves lives
Identifying patients as early as possible means that they can be monitored from then on. The hearts of some may thicken faster than the hearts of others and, if symptoms appear, they will need medical or surgical intervention.
Some patients also face a higher risk for sudden death and for them the importance of early diagnosis is clear. Their clinical team can capture timely information through echocardiograms, exercise testing, ECG monitoring and MRI to decode who is at highest risk of such an event. An ICD can be provided in a timely manner that, in the case of a dangerously bad heart rhythm, can convert it to a normal rhythm.
As such, Dr. Mital hopes that this new evidence will help to change international practice guidelines and, as a result, ultimately save lives.







 ‘A disease of all ages’
‘A disease of all ages’