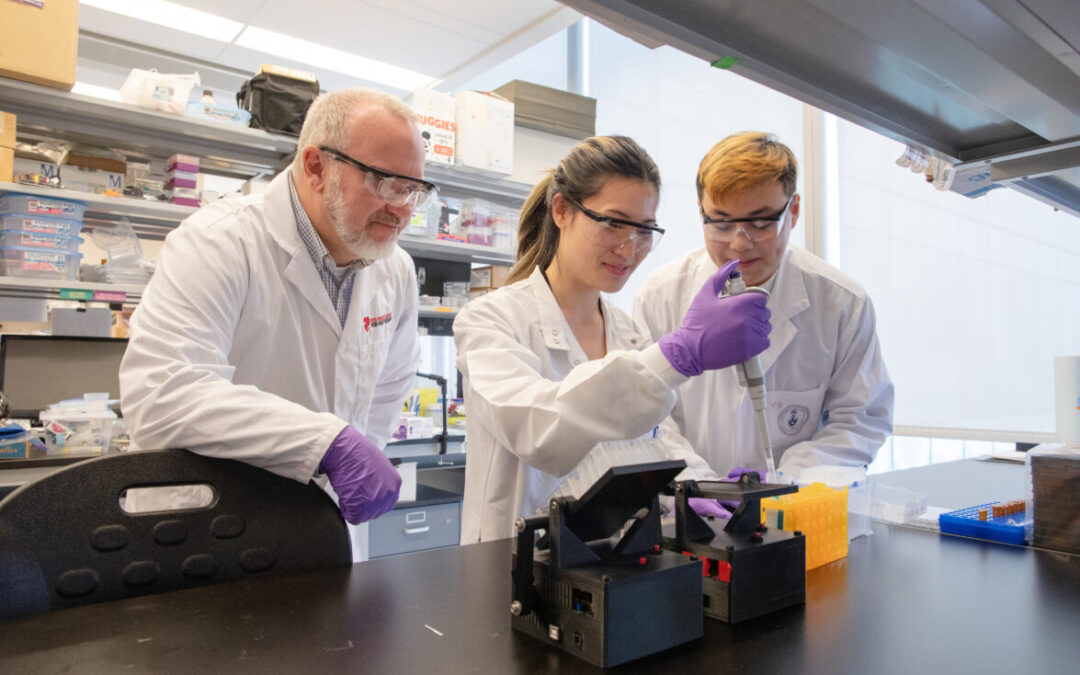
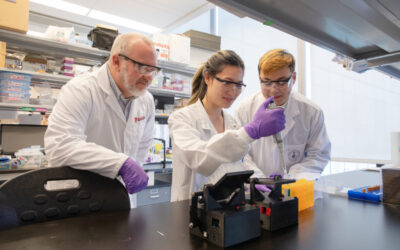
For researchers studying heart disease, lab-grown heart cells are an essential tool. Created from human stem cells, they offer a powerful way to model disease, test therapies, and better understand heart function. However, the challenge remains that these cells behave...
For children living with cardiomyopathy, heart failure is not always caused by the heart losing its ability to pump. In many cases, the problem is more subtle, but just as serious: the heart becomes stiff and struggles to relax and fill properly between beats. This...
New findings from the UNEARTH CVD research team have shed light on an important but often overlooked aspect of cardiovascular care: the cognitive health of people living with heart failure. Published in Cureus, this new publication is the first study to examine...
The Ted Rogers Centre for Heart Research is proud to celebrate an extraordinary milestone in the career of Dr. Paul Santerre, who has been elected as a Fellow of the National Academy of Inventors (NAI), the highest honour bestowed upon academic inventors. This...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
Entrepreneurship for Cardiovascular Health Opportunities (ECHO) is a 12-month national training program supporting cardiovascular research commercialization through education, mentorship, networking, and funding. Led by a diverse team of experts, ECHO fosters...
3D models of heart failure… stiffened hearts in diabetes…. saving infant lives
After a heart attack, this peptide protects the heart from further injury
Featured Event
2026 Heart Failure Symposium
Virtual Library
Visit our YouTube channel filled with world-class heart failure educational sessions on diverse topics
Investigating Heart Failure
Personalized Medicine
Equitable Access to Care
Translating Innovation
For Patients
For Clinicians
For Researchers
How one immune cell protects against heart failure
In an important recent paper published in Immunity, Ted Rogers Centre member Dr. Slava Epelman breaks new ground in world-leading research on immune cells that live in the heart.
“If you compare this to research into the immune system in other organs, this is an underappreciated field of study,” says Dr. Epelman, clinician scientist at UHN and U of T. “Comparatively speaking, we know very little about the immune cells in the heart despite the widespread impact of cardiovascular disease.”
Target: Dendritic Cells
The new study – which comprised many researchers in the Epelman lab including Xavier Clemente-Casares and Siyavash Hosseinzadeh – has two components. The first: understand the type of immune cells inside our hearts, and how they may contribute to heart failure.
The team wanted to see if the heart contains dendritic cells, which initiate the body’s T-cell immune response to defend against infection. First they discovered many types of dendritic cells inside the myocardium (muscular tissue of the heart). Then they discovered that these cells behave differently in the heart than they do elsewhere.
This suggests that the heart provides different signals when recruiting and differentiating these key cells, as compared to other organs. This means, for instance, that it can help determine which treatments can be effective and also which can be counterproductive to a patient.
Target: Viral Infections of the Heart
The study’s second component was understanding exactly how heart failure develops after a viral infection in the heart (viral myocarditis).
Because there existed no precise tools to study how T cells activate after a virus sets in, the team developed some. Through this effort, they discovered that one particular subset of dendritic cells played a critical role. In a mouse model, they found that without these dendritic cells performing that role, what was a mild infection escalated into severe heart failure. Thus, this dendritic cell subset is clearly part of a surveillance system that ensures subtle infections in heart tissue don’t worsen and evolve into significant damage.
“We have for the first time identified what immune cells serve in in this capacity, and also assessed their function and role in heart failure following viral infection,” says Dr. Epelman.
A clinical curiosity
There are no approved treatments for viral myocarditis, nor effective ways to diagnose it. In heart failure patients, it’s hard to know if an earlier infection contributed to the disease. Meanwhile, other individuals walk around with viruses in their hearts but don’t develop heart failure. Why?
As a clinician-scientist, Dr. Epelman carries a unique vantage point. He sees patients at Peter Munk Cardiac Centre with viral infections of the heart, including those who have had it before. “I wonder what the relationship is,” he wonders. “We don’t have tests to figure it out. It’s a clinical curiosity: we simply don’t know what’s at play here.”
Dr. Epelman speculates that a viral infection may be a very significant contributor to heart failure. Since the heart was infected previously, it is now vulnerable for another infection, which again puts the heart at risk.
An important note is that in half of all heart failure cases, atherosclerosis is not the culprit. In these cases, high blood pressure and a prior viral infection are major risk factors.
For this reason, his lab continues to focus on an under-appreciated area of study that may lead to newfound preventative strategies for millions of people.